Наследственные нарушения строения тканей зуба
Зачастую некариозные поражения тканей зуба развиваются не вследствие внешних воздействий или системных заболеваний, а являются результатом наследственного фактора. Развитие эмали нарушается из-за патологических изменений, которые претерпевают эктодермальные клеточные образования,а следствием этого становится атипичное строение дентина.
Несовершенный амелогенез может быть причиной внутреннего окрашивания, подробнее об этом на вебинаре Обзор техник отбеливания зубов: лазерное отбеливание, отбеливание светом, домашнее и офисное отбеливание.
Выделяют следующие виды наследственных поражений зубов:
- несовершенный амелогенез;
- несовершенный дентиногенез;
- синдром Стентона – Капдепона;
- несовершенный одонтогенез;
- мраморная болезнь;
- гипофосфатезия.
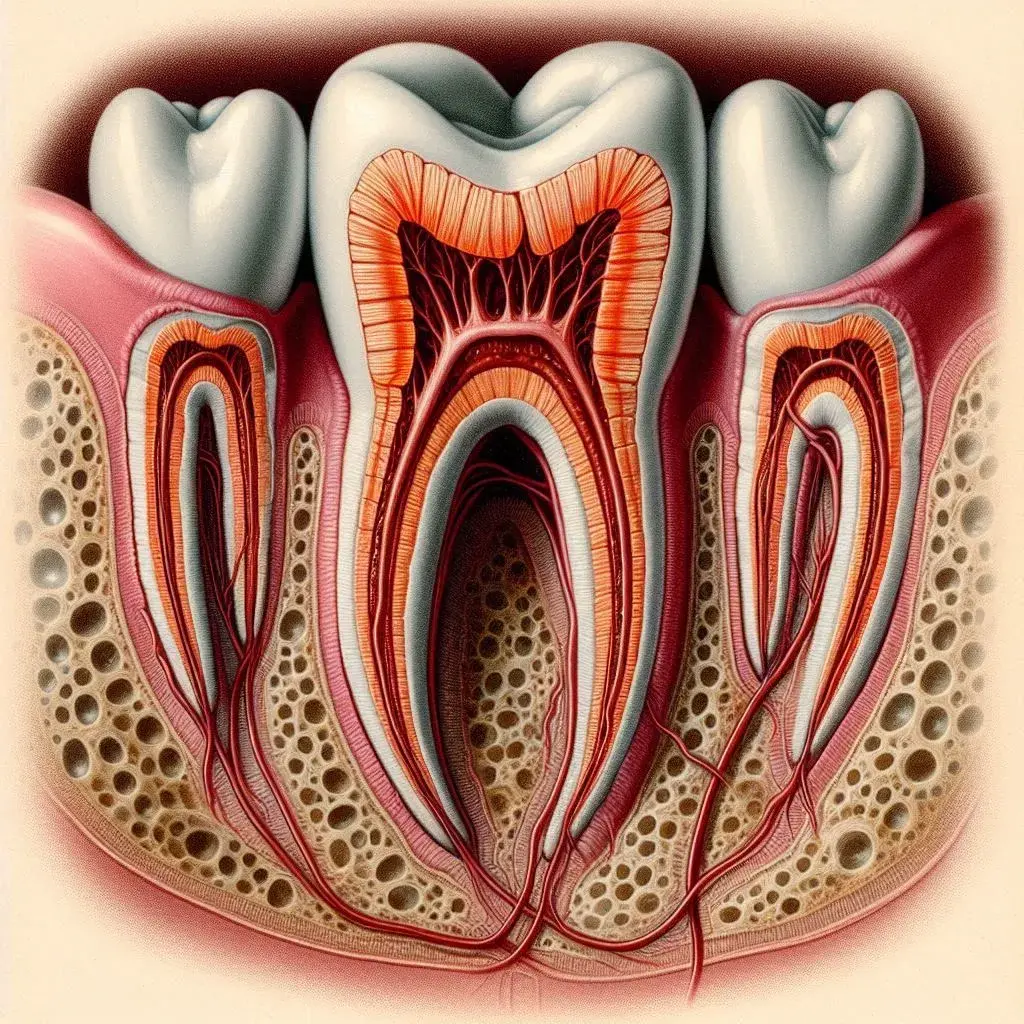
Рисунок 1. Нормальное строение тканей зуба.
Несовершенный амелогенез: клиника и классификация
Представляет собой обусловленную наследственной природой патологию развития эмали. Клиническая картина определяется качественными и количественными поражениями эмали. Принято выделять несколько вариантов несовершенного амелогенеза.
- При первом варианте наблюдаются малочисленные, часто незначительные нарушения эмали. С одинаковой частотой встречается среди представителей обоих полов. Это практически здоровые пациенты, у которых зубы прорезываются своевременно, но, как правило, коронки отличаются уменьшенными размерами. Вследствие снижения ширины коронок появляются тремы между зубами. У таких зубов эмаль сохраняет блеск и гладкость, но приобретает желтоватый или коричневый оттенок. Разные участки одного зуба могут быть окрашены в разные цветовые оттенки. Корень зуба имеет обычную конфигурацию и длину. Полость зуба и просвет каналов четко визуализируются на рентгенограмме.
- Для второго типа наследственного поражения эмали характерны более существенные количественные и качественные преобразования. Данная патология встречается с одинаковой частотой среди представителей обоих полов. Зубы прорезываются своевременно, но у коронок ширина больше в области шеек либо одинаковая во всей длине, при первом варианте коронки имеют коническую форму, а при втором – цилиндрическую. Поверхность зуба шероховатая поскольку эмаль встречается в виде отдельных островков, преимущественно в пришеечной области. Зубы окрашиваются в желтые и коричневые оттенки. Вестибулярная поверхность более пораженная относительно оральной. Патология связана со структурными нарушениями эмали, слабой ее минерализацией. Дентин имеет обычное строение. Корни обычной конфигурации и размера, полость зуба и просветы каналов четко прослеживаются на рентгенограмме. Может появляться повышенная чувствительность к некоторых раздражителям, чаще температурным и механическим. У коронок зубов на рентгенограмме неровные контуры, это обусловлено отсутствием эмали на данных участках.
- При третьем варианте несовершенного амелогенеза зубы имеют обычные размеры, форму и цвет, но в некоторых случаях эмаль истончена и оттенок ее изменен. Но в обоих вариантах поверхность зуба испещрена бороздками, которые придают рифленый вид эмали. Бороздки на поверхности в отличие от системной гипоплазии имеют не горизонтальное, а вертикальное направление. Поражены все зубы и молочные, и постоянные. Локализация бороздок по всей поверхности коронки. На рентгенограмме конфигурация корней, просвет полости зуба и каналов четко прослеживаются. На коронках определяются разной плотности, длины и ширины полоски, которые направлены от режущего края к шейке.
- При четвертом типе поражения коронки отличаются обычными размерами, имеют правильную форму, только эмаль теряет блеск, становится меловидной. Ученые считают, что это обусловлено отсутствием кутикулы и пелликулы – типичных для эмали органических оболочек. Эмаль не способна противостоять механическому влиянию и при малейшей травме отслаивается от дентина. Обнажившийся дентин сперва желтый, затем приобретает коричневое окрашивание вследствие проникновения пигмента. По мере стирания и скола эмали меняется размер и конфигурация коронок. Наблюдается повышенная чувствительность открывшегося дентина к термическим раздражителям.

Рисунок 2. Гипоплазия эмали.
Электровозбудимость пульпы в норме. Форма корней, полости зуба, просветы каналов также в пределах нормы, только на апроксимальных поверхностях видны просветления, напоминающие кариозные полости, что соответствует зонам с утраченной эмалью.
Несовершенный дентиногенез: симптомы и рентген-признаки
Представляет собой наследственную патологию развития дентина, характерна для представителей обоих полов.
Типичные клинические проявления
- Обычный размер, цвет и форма коронок зубов.
- Кариозному процессу такие зубы подвержены редко.
- Частая жалоба на боль от термических раздражителей.
- У пациентов часто отмечаются заболевания пародонта, начиная от катарального гингивита, заканчивая подвижностью зубов (преимущественно передних) на фоне отсутствия пародонтальных карманов.
- Число подвижных зубов с возрастом увеличивается, отдельные зубы выпадают.
- Корни укорочены, верхушки их заострены. В многокорневых зубах область фуркация располагается дальше от шейки зуба, на верхушках корней определяются заостренные выступы.
- Просвет каналов часто не просматривается. Сужение полости зуба и просвета каналов является пороком развития зуба.
- На верхушках корней отмечаются зоны разрежения костной ткани, с возрастом такие очаги появляются у большинства зубов.
- На шлифе зуба в пришеечной зоне выявляется резкая волнистость эмалево-дентинной границы. Строение эмали не нарушено. Слой дентина истончен, напоминает интерглобулярный дентин. В зоне режущего края выявляется интерстициальный дентикль. Полость зуба заполнена дентиклами, между ними находятся щели, в которых расположена пульпа.
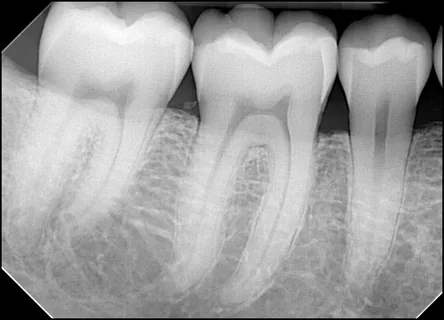
Рисунок 3. Рентгенограмма зубов.
Несовершенный одонтогенез: клиника и гистология
Представляет собой наследственное заболевание, которое чаще проявляется среди мальчиков. В основе заболевания – недостаточная минерализация формирующихся костей, в том числе тканей зуба. На рентгенограмме определяется чрезмерно тонкий кортикальный слой, губчатое вещество имеет крупноячеистое строение.
Зубы обычной величины, нормальной формы. Окраска коронок вариабельна: от серой до желтовато-коричневой, характерна повышенная просвечиваемость. Гистологическое исследование подтверждает нормальное строение эмали, но эмалево-дентиная граница напоминает прямую линию. Строение плащевого дентина правильное, по мере приближения к пульпе уменьшается количество дентинных трубочек, просвет их местами сужен или облитерирован. Дентин слабо минерализован.
Системные наследственные заболевания с поражением зубов
Мраморная болезнь
Заболевание характеризуется полным или частичным склерозированием во всем скелете губчатого костного вещества. На ранних этапах болезни склерозирование костей отмечается исключительно в области метафизов, а также в периферических отделах плоских костей. Неравномерно уплотняются кости черепа. Обычно склерозированы придаточные пазухи. Нарушение развития челюстных костей сопряжено с патологией развития и сроками прорезывания зубов. Под влиянием заболевания зубы медленно развиваются, поздно прорезываются и строение их нарушено:
- корни недоразвиты, каналы и полость зуба облитерированы;
- зубы не способны сопротивляться кариозному процессу.

Рисунок 4. Исправление формы коронок при помощи мостовидного протеза.
Гипофосфатезия
Это наследственное заболевание, относящееся к группе нарушений обмена. В основе патогенеза – врожденная патология выработки щелочной фосфатазы. Диагноз ставится при рождении ребенка, либо в течение первого полугода жизни. Типичные клинические проявления: деформации конечностей, нарушение обызвествления костей свода черепа, патологические переломы, цианоз, диспноэ, рвота, запоры, судорожный синдром, ломкость волос и ногтей.
Со стороны зубочелюстной системы:
- гипоплазия эмали;
- нарушение развития корней зубов, ускоренное рассасывание их;
- ранняя потеря зубов.
На рентгенограмме определяется несостоятельность альвеолярного отростка, рассасывание корней временных зубов, остеопороз челюстных костей.
Дисплазия Капдепона (синдром Стентона-Капдепона)
Для данного заболевания характерна нормальная форма и величина зубов, окраска вариабельна, сроки прорезывания средние. Эмаль скалывается почти сразу после прорезывания. Обнажившийся дентин усиленно стирается. Интенсивность стирания определяется выраженностью структурных изменений.
Зубы практически не реагируют на различные раздражители. Корни имеют обычную форму и длину. Полость зуба и просвет каналов сильно сужены, часто не визуализируются на рентгенограмме.

Рисунок 5. Важно раннее выявление и лечение наследственных поражений зубов.
Принципы лечения наследственных нарушений строения зубов
В основе терапии наследственных нарушений эмали зубов лежит покрытие их коронками, выбор материала зависит от групповой принадлежности зуба. В случае наследственной патологии дентина, сопровождающейся потерей зубов, показано съемное протезирование. При частичном стирании зубы покрываются искусственными коронками, в случае полного стирания применяются съемные протезы. В случае потери нескольких зубов рекомендуются мостовидные протезы.
Подробная информация о форме и пропорциях зубов на вебинаре Дентальная эстетика.