Эминектомия височно-нижнечелюстного сустава
Машинный перевод
Оригинальная статья написана на языке PT (ссылка для ознакомления) .
Введение
Височно-нижнечелюстной сустав (ВНЧС) считается одним из самых сложных в человеческом теле. Костные структуры ВНЧС — это гленоидная ямка височной кости и мыщелок нижней челюсти. У детей гленоидная ямка и суставная возвышенность уплощены, и действие функциональных нагрузок определяет морфологию ВНЧС (Liddell & Perez, 2015; Martins и др., 2014; Mayrink и др., 2012; Undt, 2011).
Во время движения открытия рта мыщелок совершает вращательное движение, а затем движение переднего смещения, идеальным образом до точки наибольшей выпуклости суставной возвышенности (Liddell & Perez, 2015; Martins и др., 2014; Mayrink и др., 2012; Undt, 2011).
Между этими костными поверхностями располагается суставной диск, структура в форме двояковогнутого, гибкого, образованная из волокнистой хрящевой соединительной ткани, отвечающая за поглощение функциональных ударов и позволяющая движению мыщелка быть гармоничным во время открытия и закрытия рта (Pereira и др., 2021).
Выраженная анатомия суставной возвышенности может представлять собой проблему для нормального функционирования ВНЧС. В этой ситуации пациент может испытывать ограничение в движении открытия рта, так как мыщелок нижней челюсти не проходит по наклону суставной возвышенности.
В 1951 году Хильмар Мюрах ввел хирургическую технику эминиктомии; она заключается в уменьшении высоты суставной возвышенности, чтобы мыщелок мог свободно двигаться без помех во время открытия и закрытия рта (Чакраборти, 2007; Лидделл и Перес, 2015; Майринк и др., 2012; Стассен и О’Халлоран, 2011; Ундт, 2011).
Клинический случай
A. S., пациент мужского пола, 20 лет, был осмотрен на первом приеме по поводу орфасциальной боли и дисфункции височно-нижнечелюстного сустава с неясной болезненной симптоматикой средней и высокой интенсивности в шейно-лицевой области без явного триггерного фактора. Пациент описывал наличие щелчков, хрипов и повторяющиеся эпизоды блокировки во время открытия рта. Все существующие клинические состояния оказывали влияние на его качество жизни на уровне 7/10 Визуальной аналоговой шкалы (VAS).
При объективном осмотре мы наблюдаем максимальное открытие рта 14 мм без отклонений, наличие щелчков и двустороннее мышечное сокращение с: сокращением 3 степени в жевательной и височной мышцах и 2 степени в грудино-ключично-сосцевидной мышце и переднем брюшке двубрюшной мышцы.
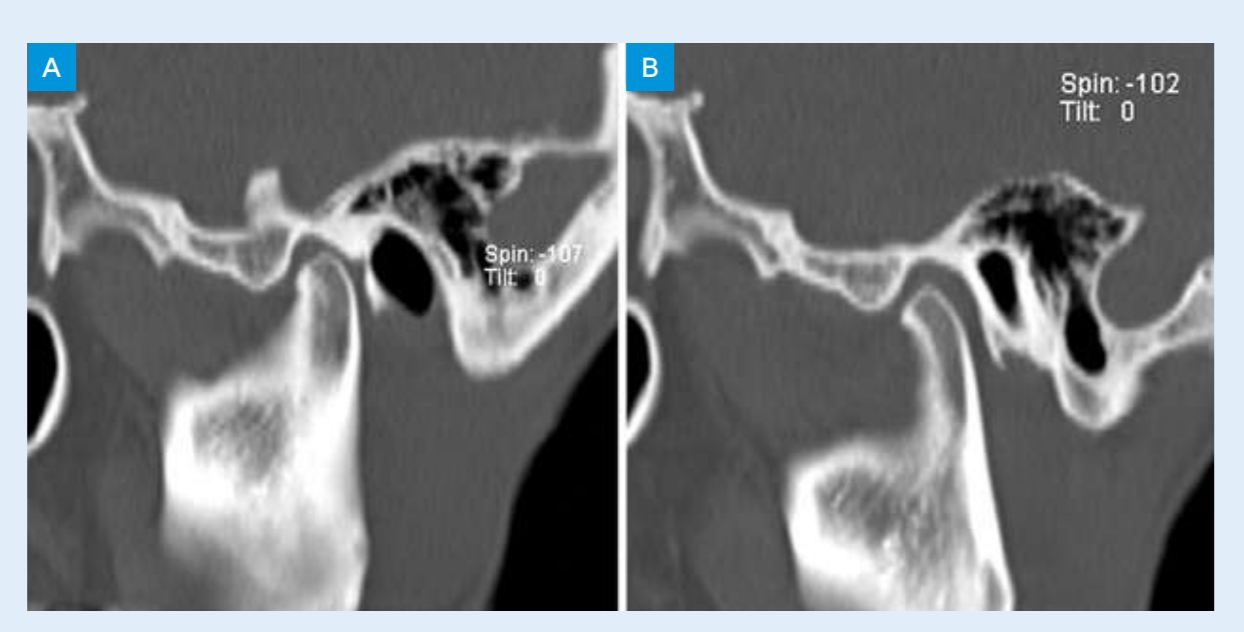
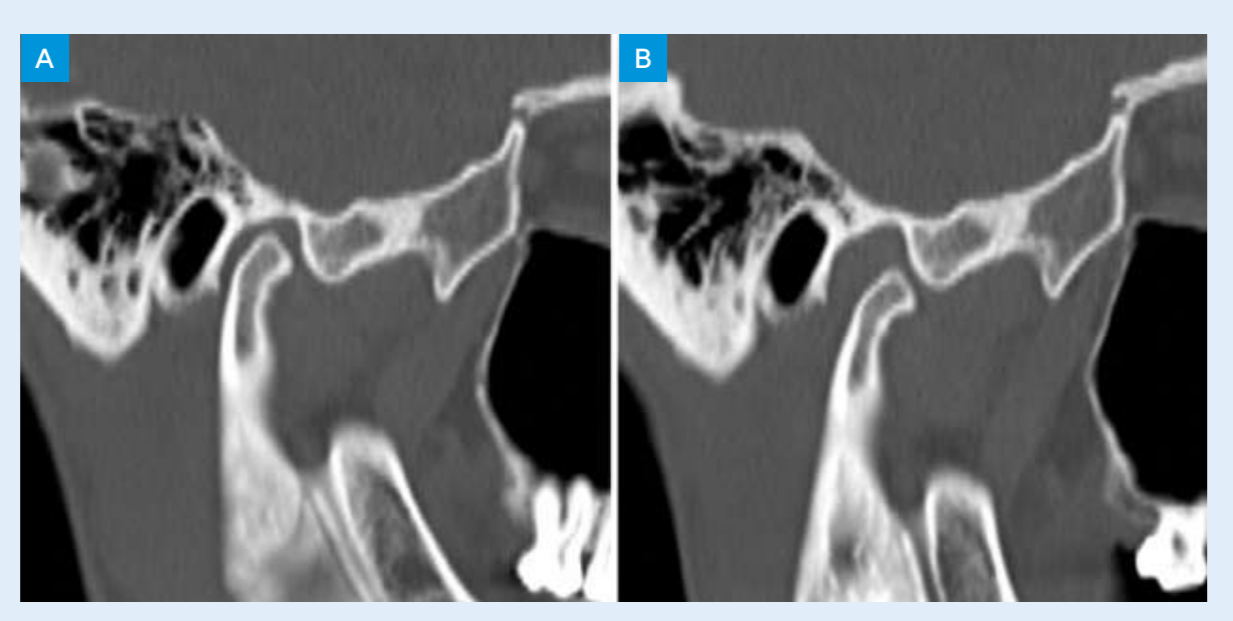
Были проведены дополнительные диагностические исследования, при этом магнитно-резонансная томография (МРТ) показала хорошее положение дисков при закрытом рте, однако при открытом рте было зафиксировано заднее смещение суставных дисков. Компьютерная томография (КТ) выявила очень острый угол суставной эминенции, который был связан с блокировкой кондилярной трансляции и задним смещением диска. На рисунках 1 и 2 можно увидеть изображения КТ при открытом и закрытом рте правой и левой ВНЧС.
Пациенту была предложена билатеральная эменектомия.
Описание хирургической техники эминектомии
Наиболее распространенным подходом при открытой хирургии ВНЧС является предушная инцизия, описанная Rowe в 1972 году. Однако, с необходимостью более эстетического подхода, она была заменена на эндоральный подход, а более недавно предложена номенклатура для модификации классического эндорального подхода: “Root of helix inter tragus notch incision (RHITNI)”. Эта инцизия выполняется с помощью лезвия 15 и проводится от нижнего края хряща до корня уха, рисуя форму V и следуя до нижнего края трагуса, заканчиваясь на вырезке уха (Ângelo, 2020).
Диссекция кожи и подкожных тканей проводилась с помощью ирисовых ножниц, до поверхностного слоя височной фасции. После хорошей экспозиции фасции она была открыта до скуловой дуги под углом 45°, чтобы минимизировать риск повреждения височной ветви лицевого нерва (см. рисунок 3). Для уменьшения суставной эминенции была выполнена маркировка остеотомии дермографической ручкой (см. рисунок 4). Уменьшение суставной эминенции было выполнено без травм с помощью пьезоэлектрического устройства (см. рисунок 5).



Закрытие хирургической раны было выполнено по слоям, с использованием шва vicryl 3/0 на уровне подкожной ткани и шва monocryl 5/0 для кожи. Для защиты также была нанесена хирургическая клей на весь шов, который был удален через двадцать дней после операции.
Вся операция прошла без осложнений, в послеоперационный период была зафиксирована максимальная открытость рта 31 мм и адекватная кондилярная трансляция.
Пациент проходил курс физиотерапии и логопедической терапии.
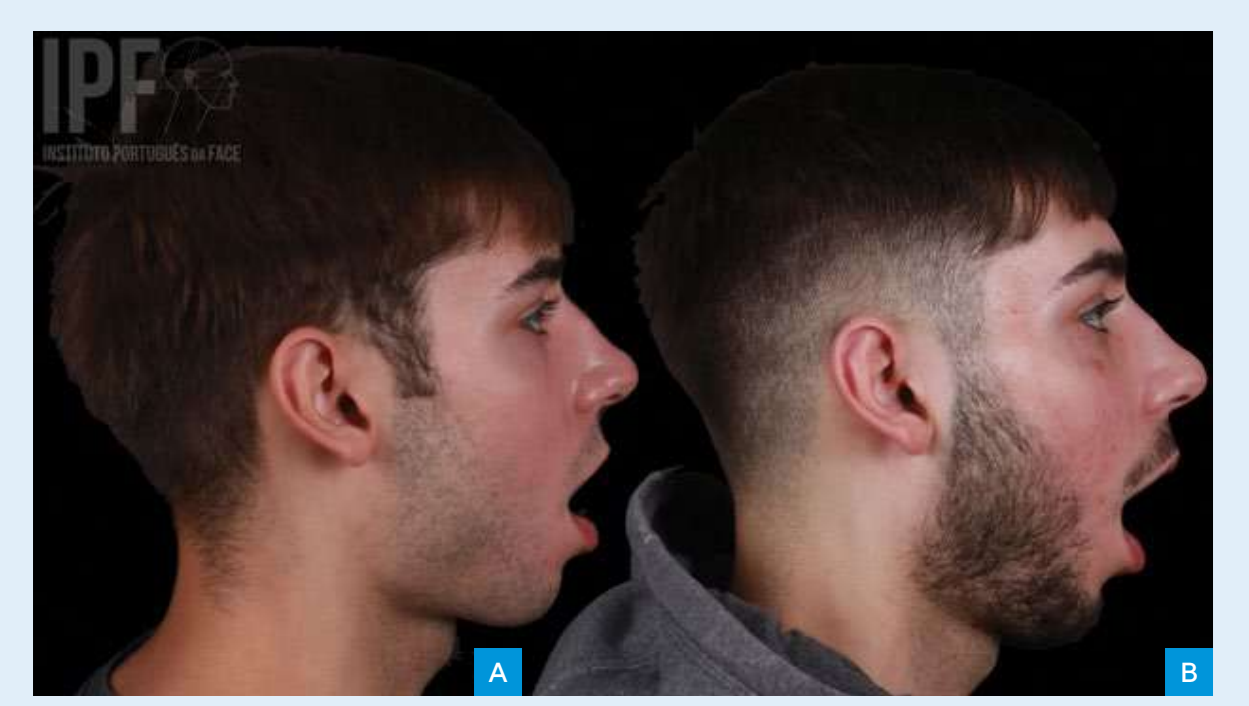
На рисунках 6(A) и 6(B) можно увидеть фотографию профиля пациента до операции и через шесть месяцев после операции при максимальном открытии рта.
Обсуждение
Эминектомия является универсальной техникой в лечении различных типов пациентов с патологией ВНЧС. Многие авторы описывают эминектомию с эффективностью 100% до 5 лет (Mayrink и др., 2012; Tocaciu и др., 2019).
Операция обычно проводится под общим наркозом, хотя некоторые авторы описывают эту процедуру, выполненную с местной анестезией и сознательной седатацией через вену (Mayrink и др., 2012; Stassen & O’Halloran, 2011).
Снижение суставной эминенции может быть выполнено с использованием долот, ротационных бор или reciprocating bone files, или, в более современном подходе, с использованием пьезоэлектрического устройства. Основное преимущество пьезоэлектрического устройства заключается в точности реза и в том, что оно является травматичным, сохраняя целостность сосудистых или нервных структур. Различные авторы также сообщили о снижении послеоперационных осложнений с использованием пьезоэлектрического устройства по сравнению с традиционной хирургией (Isler и др., 2018; Undt, 2011). Высота кости, которую необходимо уменьшить, еще не определена в научном сообществе. Некоторые авторы рекомендуют полное иссечение эминенции, а некоторые указывают только на уменьшение высоты или частичный контур эминенции (Undt, 2011). В нашем опыте проводится функциональное уменьшение эминенции, определяемое прогрессивным уменьшением до достижения идеальной трансляции.
В научной литературе описаны некоторые осложнения эминектомии, такие как повреждение лицевого нерва и тройничного нерва или повреждения соседних структур. Некоторые авторы наблюдали стойкость вывиха нижней челюсти, остеоартрит, перелом головки мыщелка, боковое отклонение при движении открытия и гипермобильность мыщелка (Isler и др., 2018; Liddell & Perez, 2015; Martins и др., 2014).
Хотя ожидается гипермобильность мыщелка из-за отсутствия суставной эминенции для ограничения движения мыщелка, исследование Undt и др. не показало изменений в суставных движениях до или после операции; авторы указывают на наличие фиброзного рубца в передней части капсулы как вероятную причину, препятствующую чрезмерному движению мыщелка. Исследование Stanssen и др. сообщает, что ни один пациент не проявил дисфункции, вызванной послеоперационной гипермобильностью. Кроме того, ни один пациент не испытывал проблем с жеванием, глотанием или речью (Mayrink и др., 2012; Stassen & O’Halloran, 2011; Undt, 2011).
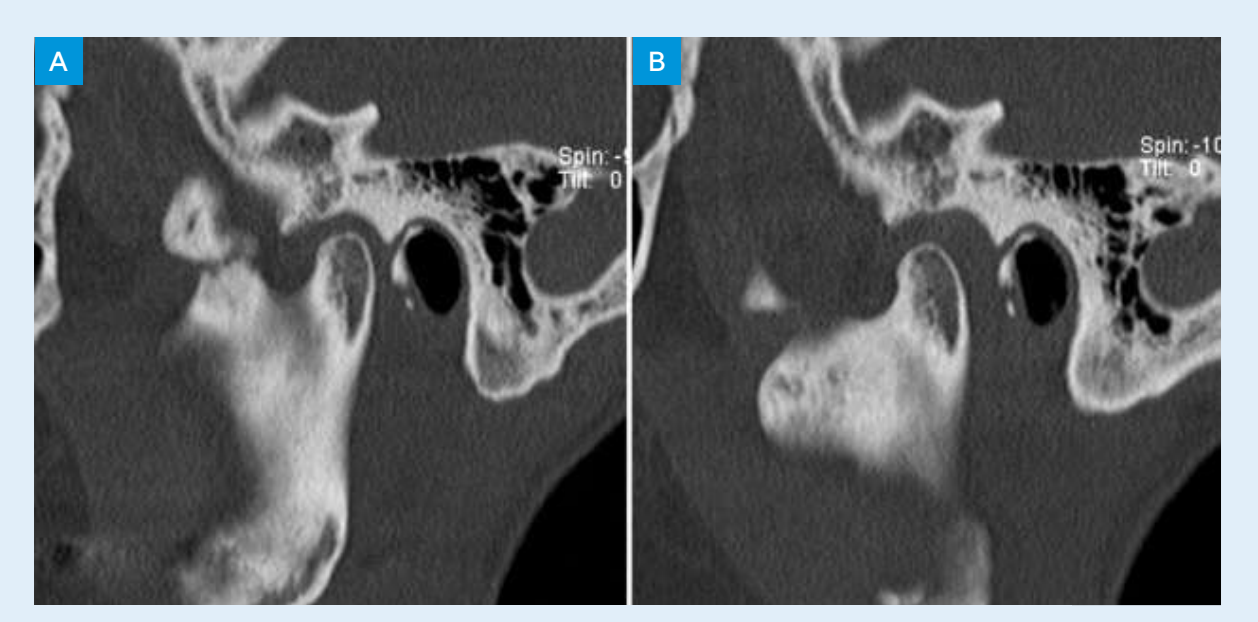
В нашем опыте наблюдалась контролируемая и ожидаемая гипермобильность, которая была решающей для улучшения открытия рта и для пассивного repositioning диска. Через год пациент прошел новое КТ, где можно было увидеть ремоделирование двусторонней суставной эминенции, как видно на рисунках 7 и 8.

Выводы
Эминектомия кажется безопасной и эффективной техникой, связанной с быстрой функциональной реабилитацией с минимальным эстетическим воздействием благодаря развитию хирургических техник.
Давид Âнгело, Давид Санз, Руте Маркес
Библиографические ссылки:
- Ângelo, D. F. (2020). Письмо редактору по теме «Корень спирали межтрагусного разреза (RHITNI) для открытой хирургии височно-нижнечелюстного сустава». В International Journal of Surgery (Том 83, стр. 233–234). Elsevier Ltd. https://doi.org/10.1016/j.ijsu.2020.09.051
- Chakraborty, C. S. K. (2007). Эминеэктомия для лечения закрытого замка височно-нижнечелюстного сустава. Медицинский журнал вооруженных сил Индии, 63(4), 384–385. https://doi.org/10.1016/S0377-1237(07)80031-1
- Isler, S. C., Cakarer, S., Yalcin, B. K., & Sitilci, T. (2018). Лечение двустороннего хронического вывиха височно-нижнечелюстного сустава. Анналы челюстно-лицевой хирургии, 8(1), 154–157. https://doi.org/10.4103/ams.ams_142_17
- Liddell, A., & Perez, D. E. (2015). Вывих височно-нижнечелюстного сустава. В Oral and Maxillofacial Surgery Clinics of North America (Том 27, Выпуск 1, стр. 125–136). W.B. Saunders. https://doi.org/10.1016/j.coms.2014.09.009
- Martins, W. D., de Oliveira Ribas, M., Bisinelli, J., França, B. H. S., & Martins, G. (2014). Рецидивирующий вывих височно-нижнечелюстного сустава: Обзор литературы и два клинических случая, леченных эминеэктомией. В Cranio: Journal of Craniomandibular & Sleep Practice (Том 32, Выпуск 2, стр. 110–117). Chroma, Inc. https://doi.org/10.1179/0886963413Z.00000000017
- Mayrink, G., Olate, S., Assis, A., Sverzut, A., & de Moraes, M. (2012). Рецидивирующий вывих нижней челюсти, леченный эминеэктомией. Journal of Craniofacial Surgery, 23(5). https://doi.org/10.1097/SCS.0b013e31825ab523
- Pereira, J. V. C., Campos, G. S., & Paula, D. M. de. (2021). Хирургический подход к нарушениям височно-нижнечелюстного сустава (TMJ): обзор литературы. Research, Society and Development, 10(13), e568101321711. https://doi.org/10.33448/rsd-v10i13.21711
- Stassen, L. F., & O’Halloran, M. (2011). Функциональная хирургия височно-нижнечелюстного сустава с сознательной седацией для «закрытого замка» с использованием эминеэктомии в качестве лечения: серия случаев. Journal of Oral and Maxillofa- cial Surgery, 69(6). https://doi.org/10.1016/j.joms.2010.11.034
- Tocaciu, S., McCullough, M. J., & Dimitroulis, G. (2019). Хирургическое лечение рецидивирующего вывиха TMJ — систематический обзор. Оральная и челюстно-лицевая хирургия, 23(1), 35–45. https://doi.org/10.1007/s10006-019-00746-5
- Undt, G. (2011). Эминеэктомия височно-нижнечелюстного сустава для рецидивирующего вывиха. В Atlas of the Oral and Maxillofacial Surgery Clinics of North America (Том 19, Выпуск 2, стр. 189–206). https://doi.org/10.1016/j.cxom.2011.05.005
- Vyloppilli, S., Joseph, B., Manojkumar, K. P., Sayd, S., & Krishnakumar, K. S. (2017). Хирургическая коррекция двустороннего вывиха TMJ с эминеэктомией и капсулоррафией в качестве адъюванта: клинические случаи. Журнал челюстно-лицевой и оральной хирургии, 17(3), 345–349. https://doi.org/10.1007/s12663-017-1030-y