
en
Salivary stone disease. Clinic and diagnostics
119
10 мин чтения
16 января 2024
Машинный перевод
Оригинальная статья написана на языке RU (ссылка для ознакомления).
Synonyms for this disease are sialolithiasis and calculous sialadenitis, which was previously considered a rather rare pathology. However, today salivary stone disease is the most common lesion of the salivary glands, with an incidence of about 35-75%.
The submandibular salivary glands are most often susceptible to the formation of stones; they account for 95% of cases of the disease, less often - the rest. It is extremely rare for stones to form in children. There are no differences by gender, but among the urban population the disease occurs many times more often than among residents of rural areas.
All necessary protocols for the diagnosis and treatment of inflammatory diseases of the maxillofacial area in the online course Treatment of inflammatory diseases of the maxillofacial area: new approaches .
Etiology and pathogenesis
The nature of the disease is multifactorial; to date, only the mechanism of pathogenesis has been established for certain. Microsialoliths are normally continuously formed in the salivary gland, but they are freely washed out along with salivary secretions into the oral cavity.
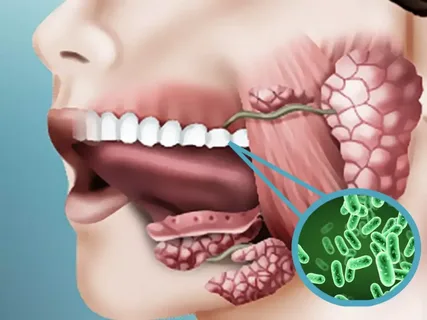
Rice. 1. Microbial invasion as the cause of the development of salivary stone disease.
The formation of stones is based on a congenital pathology of the salivary gland, which is accompanied by local dilations of the ducts of different levels and an atypical configuration of the main duct, which takes on the appearance of a broken line with sharp and frequent bends, where stone formation occurs. In case of disruption of the secretory function of the salivary gland, hyposalivation, saliva with microsialoliths is retained and accumulates in the enlarged areas of the ducts.
Additional factors that contribute to stone formation and subsequent stone growth:
impaired mineral metabolism;
lack of vitamin A;
contamination of the excretory duct with microorganisms or penetration of a foreign body into it;
chronic sialadenitis, which the patient suffers from for a long time.
In some cases, the formation of calculi in the salivary gland can be associated with insufficient production of statherin, which is an inhibitor of calcium phosphate precipitation.
Composition of salivary stone:
an organic component making up 75-90% of the mass, its qualitative composition resembles tartar,
mineral component.
Stone structure
The core, located in the center, is represented by organic contents: desquamated epithelium lining the ducts of the gland, salivary blood clots, microorganisms, actinomycetes, leukocyte accumulations. May present as a foreign body.
A layered substance formed by spherical bodies is located around the core. Scientists associate the layered structure of the salivary stone with various rhythms that affect the patient’s body.
Rice. 2. Location of the parotid salivary gland.
Clinical picture
The presence of certain symptoms in a patient is determined by the stage of the disease, the configuration and location of the salivary stone, the reactive forces of the body and other factors.
Stages of salivary stone disease:
initial;
stage of clinical manifestations;
late.
Key symptoms of salivary stone disease
pain syndrome, which is provoked by eating, and sometimes by the type of salty food,
swelling on the affected side of the gland.
The nature of the pain syndrome is influenced by the location of the stone, its configuration and mobility. When the stone is motionless and located in such a way that it does not interfere with the movement of saliva, the patient may not experience pain at all. Such a stone is called mute.
At the initial stage of stone formation, the patient has no complaints, salivation during this period is normal, and there are no pronounced inflammatory changes in the gland. The presence of a calculus at this stage can only be determined by chance, as a result of an X-ray examination, which was performed for other indications.

Rice. 3. Pain and swelling are the main symptoms of SCD.
The appearance of the first symptoms is associated with a disturbance in the flow of saliva, which is provoked by the intake of sour and spicy foods. The patient complains of the sudden appearance of a painful swelling, dense to the touch, which forms in the area of the affected salivary gland.
The addition of pain during eating is caused by stretching of the gland due to the blocking of the lumen of the duct by a calculus, which prevents the release of saliva into the oral cavity. At the end of the meal, swelling and pain disappear.
In some cases, the pain syndrome has a paroxysmal nature, which is not associated with food. The intensity of pain during salivary colic can vary. Periods of exacerbation are followed by periods of remission of the disease, which can last for months and sometimes years. Gradually, the damage to the gland progresses, the disease enters a late stage.
Diagnostic features
The basis of the diagnosis of calculous sialadenitis is not only the fact of identifying the presence of a stone, studying its location, shape and size, but also finding out the cause of its formation, predisposing factors and the possibility of relapses. During the diagnostic process, it is also very important to establish the functional state of the affected gland.
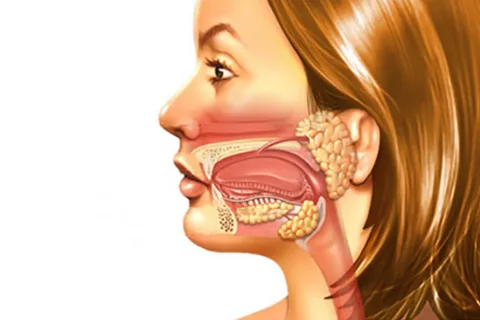
Rice. 4. Location of the salivary glands.
Diagnostic methods include the following:
duct probing;
qualitative and quantitative study of saliva;
sialography;
plain radiography;
cytological examination of saliva;
computed sialotomography;
echosialography.
A very important complaint that should be clarified from the patient during medical history is an increase in the size of the gland that occurs when eating.
If the calculus is located in the submandibular salivary gland, it can be easily identified using bimanual palpation, moving along the main duct. It is possible to palpate small stones only if they are located in close proximity to the mouth of the duct.
When performing palpation of the submandibular duct, it is important to move your fingers from back to front, this will avoid displacement of the stone into the intraglandular portion of the duct.
If the suspected calculus is localized in the anterior section of the excretory duct of the parotid salivary gland, it is recommended to palpate it from the side of the buccal mucosa; in the case of masseterial location, it is determined from the skin.
It is important to take into account the fact that the detection of compaction during bimanual palpation may indicate not only calculous sialadenitis, but also be a symptom of chronic infection, polymorphic adenoma, lymphadenitis, phlebolitis, amyloidosis.
Probing the duct is a diagnostic procedure that allows one to reliably determine the presence of a stone and calculate the distance from the mouth of the duct to the stone. A contraindication for this manipulation is exacerbation of sialadenitis, since it can provoke perforation of the duct wall.
For probing, salivary probes are used, which are available in various diameters. These devices are equipped with a flexible working part, and the ability to select the required diameter facilitates probing and helps determine the size of the duct orifice.
Radiography is the leading diagnostic method for treating salivary stone disease. Survey radiography of the parotid gland is performed in a direct projection, which eliminates the overlap of the skull bones and gives a complete picture of the size, topography and shape of the stone.
If it is necessary to examine the submandibular gland, a lateral projection is used.
It is not always possible to notice the shadow of a stone on an x-ray. This may be due to the overlap of bones and radiopaque stones, which is determined by their chemical structure.
To increase the accuracy of diagnosing calculous sialadenitis, sialography was proposed, which is accompanied by the introduction of radiopaque substances into the gland that are soluble in water; they do not have a traumatic effect on the gland.
Sialography allows you to identify radiopaque stones; on sialograms they represent defects in the filling of the duct.
Computed sialotomography is used to determine the spatial localization of the stone, which is important at the stage of choosing a treatment protocol.

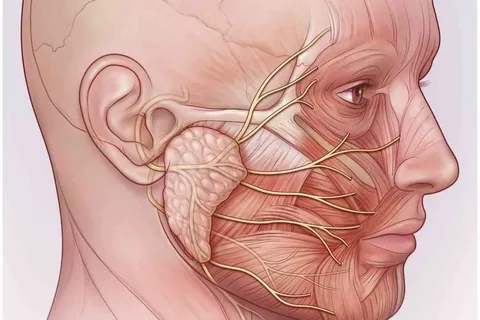
Rice. 5. The danger of surgery is nerve damage.
Treatment of calculous sialadenitis
Treatment is based, in addition to direct stone removal, on the exclusion of recurrent stone formation. The presence of a calculus in one of the intraglandular ducts entails its extirpation along with the salivary gland, which is a very labor-intensive manipulation.
Conservative methods are ineffective; they are used in the presence of a small stone localized in the immediate vicinity of the mouth of the excretory duct. Patients are prescribed a salivary diet and appropriate medications that stimulate saliva production. Small stones are thrown out by a current of saliva into the oral cavity.
Even more useful and relevant information is available in the Oral and Maxillofacial Surgery Training section of our website.