Болезни прорезывания зубов
В ежедневной практике челюстно-лицевого хирурга встречаются пациенты с аномалиями развития зубов.
К ним относятся:
- Дистопия – это зубочелюстная аномалия, которая характеризуется неправильным положением прорезавшегося зуба.
- Полуретенция – это неполное прорезывание зуба.
- Ретенция – это задержка прорезывания сформированного зуба.
Подробнее о классификации положения третьих моляров на вебинаре Удаление атипично расположенных зубов: пьезохирургический подход.
Перикоронит
Перикоронит чаще всего встречается при затрудненном прорезывании нижнего зуба мудрости, но также может наблюдаться в области верхнего зуба мудрости, премоляров и клыков на обеих челюстях. Прорезывание нижних третьих моляров происходит не ранее 18–26 лет, редко наступает раньше этого срока, чаще –позже. Особенности анатомического строения зубов мудрости разнообразны. Они, как правило, имеют сросшиеся или изогнутые корни и хорошо выраженные округлые коронки.
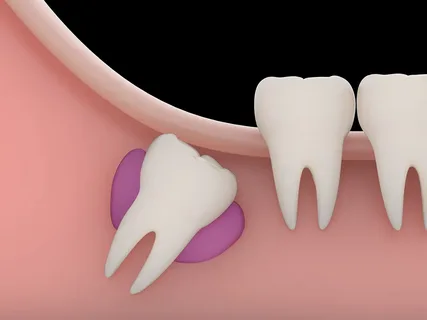
Рис. 1. Ретенция нижнего третьего моляра.
Этиология
- В области прорезывания отсутствует временный зуб, следовательно, кортикальная пластинка здесь будет максимально плотная.
- Толстая слизистая оболочка, покрывающая альвеолярную часть, включает волокна щёчной мышцы, что существенно затрудняет прорезывание.
- Недостаток места в теле нижней челюсти.
Патогенез
Когда коронка третьего нижнего моляра прорезывается и обнажаются медиальные бугры, непрорезавшиеся бугры остаются покрыты слизистой оболочкой, так называемым капюшоном. Согласно проведенным исследованиям, обсемененность слизистой патогенной микрофлорой в области капюшона зуба мудрости и позадимолярной ямки существенно выше, чем на других участках. Ситуация усугубляется травмированием отечной и воспаленной слизистой капюшона зубами-антагонистами.
Гнойная инфекция распространяется в соответствии с анатомическими особенностями строения дистального участка нижней челюсти. Так ретромолярная область богата рыхлой клетчаткой, также ее много между слизистой и волокнами щёчной мышцы, по ходу верхнего сжимателя глотки, у заднего края челюстно-подъязычной мышцы.
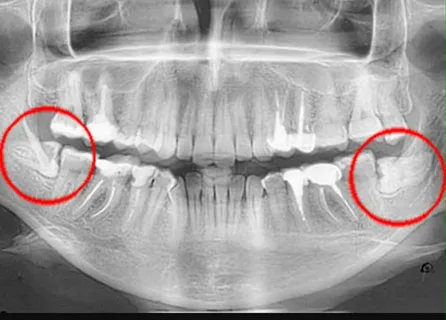
Рис. 2. Дистопия нижних зубов мудрости на рентгенограмме.
Отсюда наиболее частые осложнения:
- острый гнойный ретромолярный периостит,
- околочелюстные флегмоны и абсцессы.
Классификация
Формы затрудненного прорезывания нижнего зуба мудрости:
- острый перикоронит, может протекать в катаральной или гнойной форме;
- хронический перикоронит;
- позадимолярный периостит.
Острый перикоронит
Острый перикоронит представляет собой патологический процесс, сопровождающийся воспалением десны и краевого периодонта вокруг зуба мудрости при затруднении его прорезывания.
Этиология
Активизация естественной микрофлоры рта, где преобладают факультативные анаэробы и анаэробы.
Патогенез
- В области медиальных бугров слизистая лизируется.
- Оставшаяся часть коронки покрыта слизистым капюшоном.
- Под капюшоном и в околозубном пространстве создаются благоприятные условия для размножения микроорганизмов.
- Травмирование слизистой капюшона в процессе жевания вызывает эрозирование, ослабление местного иммунитета.
- Запускается воспалительный процесс.
Клиническая картина
Острый катаральный перикоронит. Открывание рта затруднено, болезненное жевание, температура не повышена, общее состояние не страдает. Лимфатические узлы могут увеличены, при пальпации болезненны. Открывание рта умеренно затруднено. Местно зуб находится под отечным гиперемированным слизистым капюшоном, пальпация которого безболезненная, выделения отсутствуют. Прогноз благоприятный, процесс купируется легко при своевременном лечении.
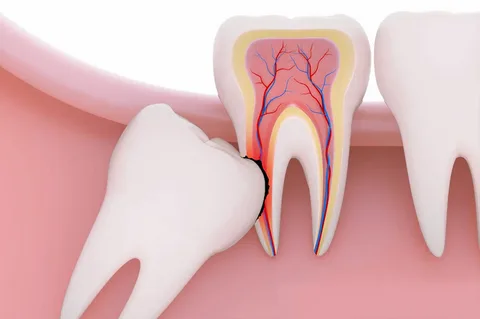
Рис. 3. Дистопия и импакция нижнего третьего моляра.
Острый гнойный перикоронит. Протекает на фоне ухудшения общего состояния организма, повышения температуры тела. Характеризуется сильной болью в дистальном отделе нижней челюсти, которая носит постоянный характер, усиливается при приеме пищи, иррадиирует в височную область, ухо. Сильная боль существенно ограничивает открывание рта. Лимфатические узлы болезненные, увеличенные. Слизистый капюшон внешне отечен и гиперемирован. При пальпации выявляется болезненный уплотненный инфильтрат, если надавить на него, появляется гнойное отделяемое.
Хронический перикоронит
Развитие хронического перикоронита происходит в результате постоянного травмирования слизистого капюшона пищей или зубом-антагонистом, вследствие частых обострений воспалительного процесса. Скопление гнойного отделяемого и образование грануляций в области капюшона вызывает местную резорбцию костной ткани.
Клиническая картина
Для хронического перикоронита характерна вариабельность клинических проявлений.
- Иррадиация боли в ухо и височную область.
- Неприятный привкус и запах из полости рта.
- Увеличение и болезненная пальпация лимфатических узлов.
- Отек и местная гиперемия слизистого капюшона.
- Серозное, а со временем гнойное отделяемое из-под капюшона при надавливании.
- Болезненная пальпация дистального отдела альвеолярного отростка нижней челюсти.
- Частые обострения процесса.
Лечение перикоронита
Терапия направлена на купирование острого процесса воспаления.
- Промывание подкапюшонного пространства растворами антисептиков.
- Рассечение слизистого капюшона вдоль, обнажение коронки, что позволяет избежать дальнейшего скопления гноя.
- Антибиотикотерапия.
После купирования острого процесса необходимо принять решение о судьбе самого зуба.

Рис. 4. Показания для удаления зуба мудрости.
Если зуб мудрости имеет правильное положение в кости и ему достаточно места для дальнейшего прорезывания, в этом случае врач полностью иссекает капюшон, целиком освобождая коронку.
Если зуб имеет неправильное положение (дистопирован) либо для его прорезывания отсутствует достаточное пространство в кости, показано его удаление.
Стоит помнить, что удаление зуба мудрости в период обострения воспалительных процессов не рекомендуется.
Позадимолярный периостит
Данный воспалительный процесс является результатом нарушения оттока гноя при перикороните, инфекция из-под капюшона распространяется под надкостницу позадимолярной ямки и клетчатку позадимолярного пространства, что приводит к образованию абсцесса.
Клиническая картина заболевания схожа с проявлениями гнойного перикоронита, только все симптомы более выражены.
- Сильная боль при открывании рта и проглатывании слюны.
- Страдает общее состояние, слабость, утомляемость, подъем температуры.
- Отек дистального отдела нижней челюсти.
- Лимфатические узлы увеличены, при пальпации болезненны.
- Открывание рта может быть полностью ограничено.
- Болезненный воспалительный инфильтрат из позадимолярной области распространяется на наружную, иногда внутреннюю поверхность альвеолярного отростка челюсти.
Принципы лечения
- Лечение в условиях поликлиники.
- Показания для удаления зуба мудрости зависят от его положения в кости и наличия места для него, но удаление производится только после стихания острого процесса.
- Разрез выполняется от крыловидно-нижнечелюстной складки, ее основания, книзу, в сторону свода преддверия рта. В случае разлитого воспаления разрез может заканчиваться на уровне моляров.
- В ране оставляют дренаж, назначают ежедневные перевязки.
- Антибиотикотерапия.
Кисты прорезывания
Согласно результатам проводимых исследований, кисты прорезывания наблюдаются в 30% случаев затрудненного прорезывания третьих нижних моляров. Считается, что причиной образования кисты является хронический перикоронит, в результате постоянного местного воспаления происходит отслаивание слизистой оболочки от зуба.
Некоторые авторы полагают, что формирование кисты прорезывания – это следствие сохранения эмбрионального эпителия, а киста является фолликулярной (содержит зуб).
Клинические проявления фолликулярной кисты в стадии обострения схожи с клиникой острого или обострения хронического перикоронита. Отличить заболевание можно по рентгенологическому снимку ветви челюсти, выполненному в боковой проекции.
Если киста небольшая, она удаляется вместе с зубом мудрости. Если ее границы распространяются на ветвь и тело челюсти, приближаются к каналу нижней челюсти, удаление кисты и зуба показано в условиях стационара.
Техника удаления дистопированных, ретенированных зубов
- Выполняется местная проводниковая анестезия.
- Оперативный доступ планируют так, чтобы минимально травмировалась кость и окружающие анатомические структуры.
- Чаще используется вестибулярный подход, реже — небный.
- Разрез слизистой оболочки должен быть достаточным для скелетирования тканей в области расположения зуба.
- Форма разреза может быть углообразная, линейная или трапециевидная.
- Слизисто-надкостничный лоскут отслаивается, костная ткань над зубом удаляется бормашиной.
- При помощи элеватора зуб вывихивается и извлекается щипцами.
- По возможности рана ушивается.
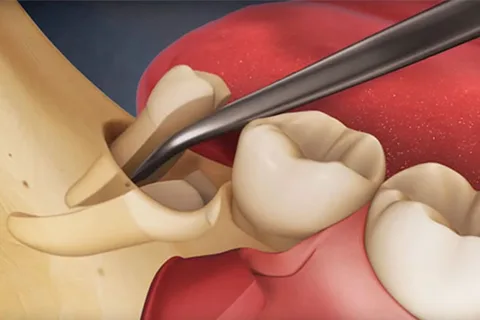
Рис. 5. Удаление нижнего зуба мудрости.
Если вам понравилась данная статья, обратите внимание на вебинар Импакция зубов: причины развития, анатомические предпосылки, инструменты и техники операций.